

Published on 20.06.2019
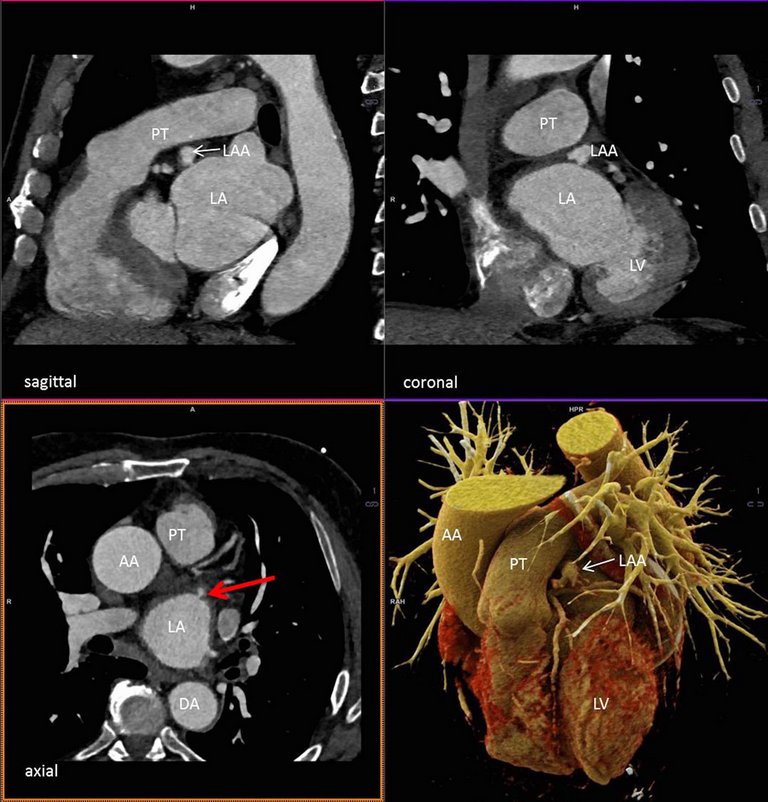
A rare entity that should be recognised by both cardiologists and radiologists to avoid misinterpretation in cardiac imaging.


Published under the copyright license.
"Attribution - Non-Commercial - NoDerivatives 4.0"
No commercial reuse without permission.
See: emh.ch/en/emh/rights-and-licences/
