

Published on 01.09.2021
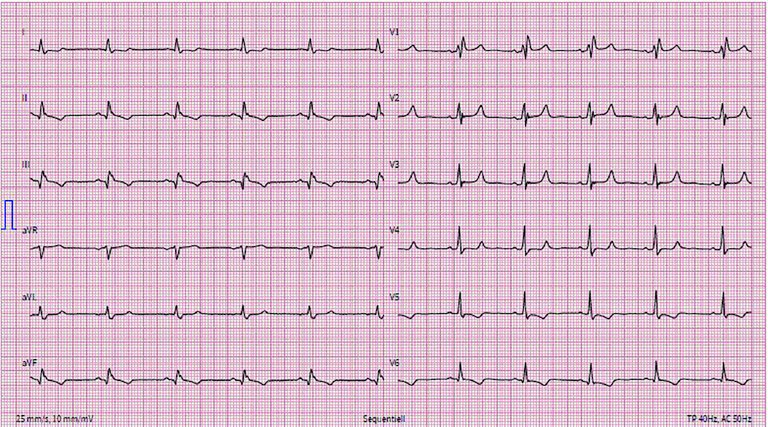
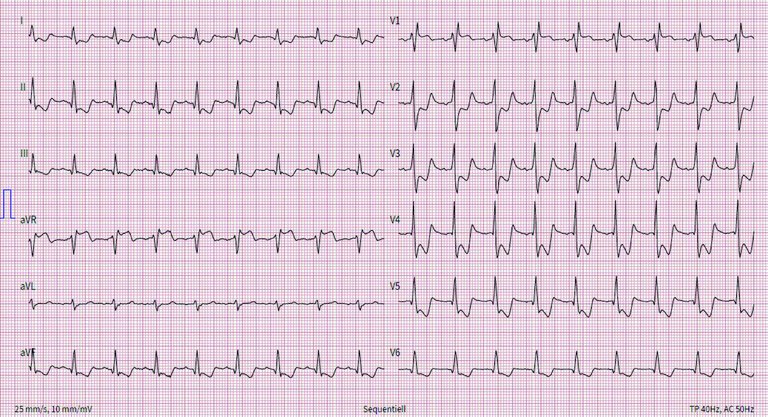
A 76-year-old male presented to the emergency room with a sudden progression of chronic intermittent retrosternal chest pain for 2 hours.
Published under the copyright license.
"Attribution - Non-Commercial - NoDerivatives 4.0"
No commercial reuse without permission.
See: emh.ch/en/emh/rights-and-licences/
