

Published on 28.02.2020
| Rule-out cut-off points (ng/l) | |||
|---|---|---|---|
| Acute heart failure | BNP | All | <100 |
| If body mass index <25 kg/m2 | <170 | ||
| If body mass index 25-35 kg/m2 | <110 | ||
| If body mass index ≥35 kg/m2 | <54 | ||
| NT-proBNP | <300 | ||
| Chronic heart failure | BNP | <35 | |
| NT-proBNP | <125 | ||
| Higher concentrations than expected | Older age |
| Chronic kidney disease | |
| Atrial fibrillation | |
| Pulmonary hypertension | |
| Pulmonary embolism | |
| Cardiac amyloidosis | |
| Severe sepsis/septic shock | |
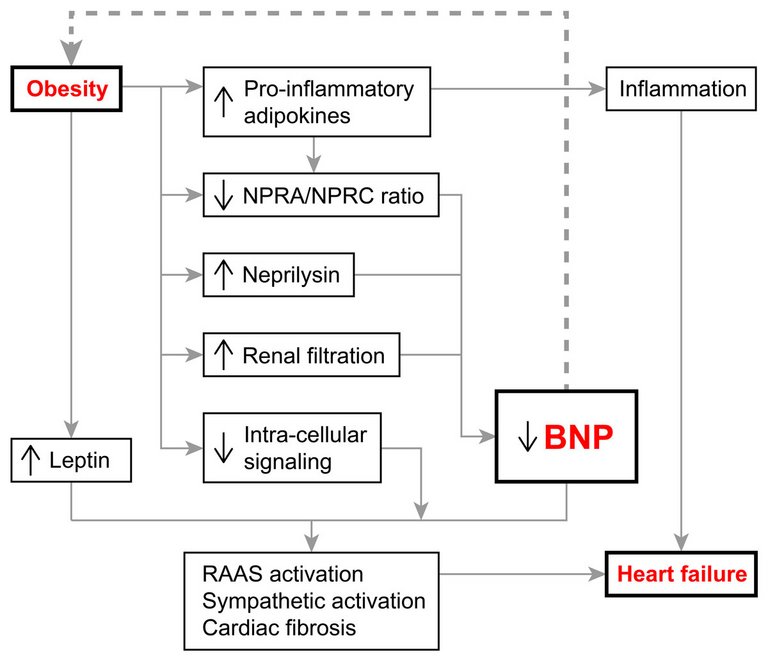
| Lower concentrations than expected | Obesity |
| Flash pulmonary oedema | |
| Cardiac tamponade | |
| Mitral stenosis |
Published under the copyright license.
"Attribution - Non-Commercial - NoDerivatives 4.0"
No commercial reuse without permission.
See: emh.ch/en/emh/rights-and-licences/
